“Quarantina” denomination), following
‘Hippocrates recommendations’. Later on, the quarantine duration was modulated according to the incubation period of the disease and the duration of the journey in. Regarding the Covid-19 pandemic, the French media thought it correct to use the neologism “quatorzaine” to designate a 14 day quarantine. In law, this term refers to “a period of 14 days to be observed legally between each step of a judiciary seizing procedure”.
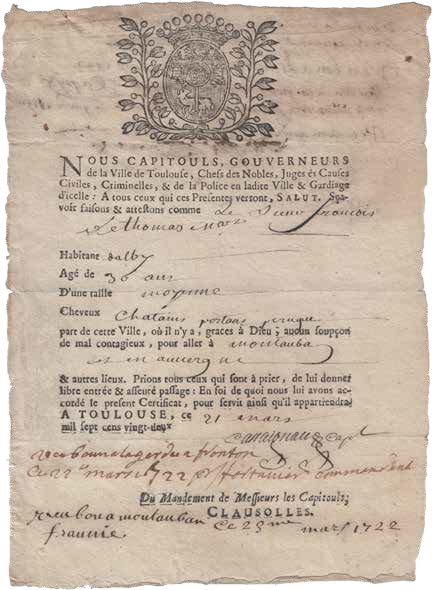
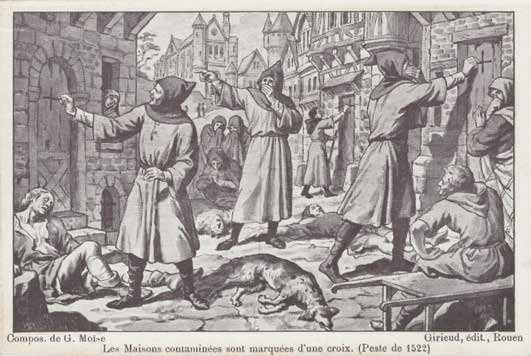
During the current pandemic, many governments have enforced ‘containment’ measures, with diverse durations and modalities according to epidemic progress. The choice between partial and total containment is a matter for much discussion which, when one considers the very fast contagion progress, can lose precious time and ground to the virus. Complying with measures restrictive to individuals but absolutely needed collectively is sometimes poorly understood, and often poorly executed, which legitimates strict control procedures, such as the use of downloadable ‘derogatory displacement authorisation’ and police controls – before possibly even more severe decisions. These measures mirror those used during ancient great epidemics: I) ‘derogatory displacement authorisations’ are the new ‘bill of health’; II) non observance of the displacement restrictions leads to fines, the value of which have rapidly increased, and soon to more coercive sanctions (jail); in the time of plague and cholera, infringements of circulation bans were punished by fines, prison, forced labor, desptach to penal colonies, or even death in the worst cases.
4. Transmission modes and risks
The French ministry for Health issued a list of Frequently Asked Questions, to be “regularly updated according to available knowledge”.
It is now established that: i) Covid-19 is a new virus ; ii) the most likely hypothesis is that of an initial transmission from animals to humans, without any more precise detail at the moment; iii) transmission between humans is certainly by respiratory inhalation (Pflügge droplets); iv) the virus killed by heat, hence possible transmission risk via raw or poorly cooked meat and/or fish.
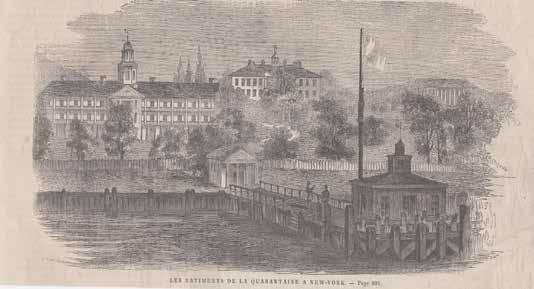
After a period of uncertainty and even downscaling (the severity of Covid-19 infection is in no way comparable to that of seasonal flu), it is now obvious that this new virus is highly contagious. Its incubation duration does not seem to exceed 14 days, which corresponds to the quarantine duration enforced by the French sanitary authorities for the French citizens isolated in Carry-le-Rouet.
The Ministry documents specify that “coronavirus Covid-19 persists up to three hours on dry inert surfaces, and up to six days in wet conditions”. Therefore, “to clean and disinfect housing occupied by persons affected by Covid-19, it is recommended to use classic cleaning and disinfection products: detergents on wet surfaces (notably sinks, showers, bathtubs and waterclosets), followed by disinfection with diluted bleach solutions as prescribed by the manufacturer”. It is best to use “single-use gloves, which should then be